
After the first 24 hours the ratio of albumin to crystalloid may be increased to establish and maintain a plasma albumin level of about 25 g100 mL or a total serum protein level of about 52 g100 mL. Colloid solutions are prepared by dissolving colloid molecules in isotonic saline solutions or more rarely in other crystalloids.

Crystalloids Vs Colloids For Fluid Resuscitation In The Intensive Care Unit A Systematic Review And Meta Analysis Sciencedirect
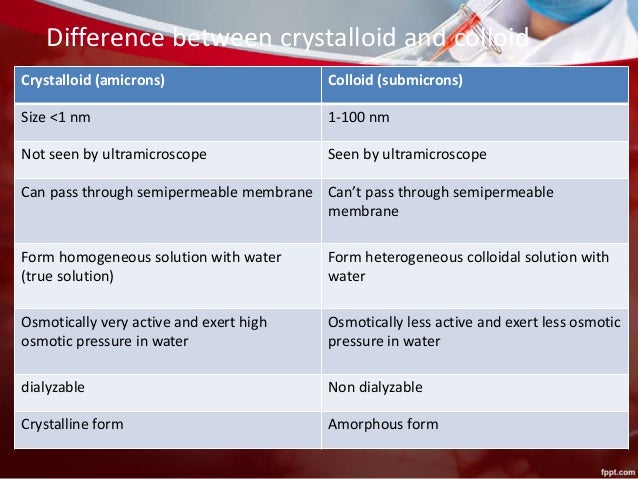
Intravenous Fluids Crystalloids And Colloids

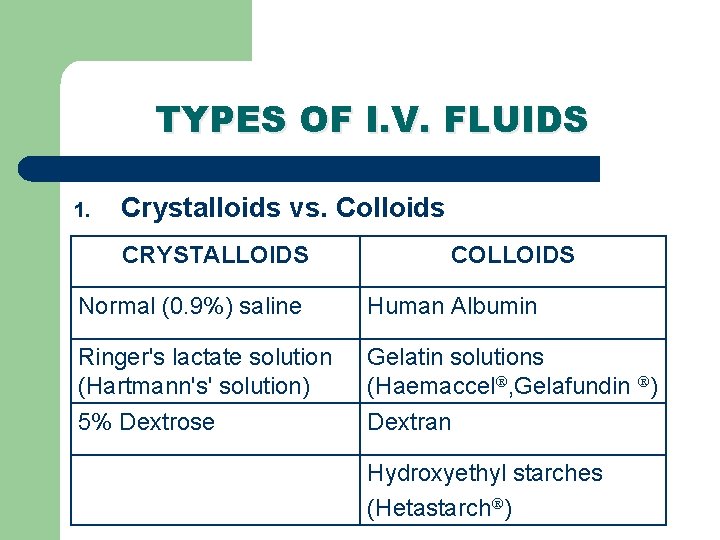
Types Of Crystalloid And Colloid Fluids
Non-balanced fluids such as normal saline NS are isotonic to plasma but do not contain the equivalent electrolyte composition.
Crystalloid and colloid fluids. D5W is initially an isotonic solution and provides free water when dextrose is metabolized. Thus albumin as an intravenous colloid solution makes perfect sense to maintain intravascular colloid pressure. Replacement of fluids intravenously resolves the imbalance and restores normal body functions.
It is an intravenous colloid that behaves much like blood filled with albumins. Crystalloid Colloid Pros and cons of each strategy Replace blood with blood Replace plasma with colloid Burns Resuscitate with colloid andor crystalloid Replace ECF depletion with saline Loss of water and salt Dehydration. What nurses need to know for more in-depth information regarding colloid and crystalloid solutions.
British Journal of Anaesthesia. Gelofusine is a colloid volume expander which may be used as a blood plasma replacement when a significant amount of blood is lost due to extreme hemorrhagia trauma dehydration or a similar event. Skytte Larsson J et al 2015 Effects of acute plasma volume expansion on renal perfusion filtration and oxygenation after cardiac surgery.
These factors provide a safety margin of about 9 times the resting oxygen requirement. Synthetic colloid preparations are less expensive than albumin and their effects can last 24 to 36 hours. A randomized study on crystalloid vs colloid.
Albumin is contraindicated in TBI and HES and other starches are not recommended 293031. Hypotonic solutions such as 045 sodium chloride solution arent appropriate for. Some crystalloid solutions are used in specific circumstances to replace electrolyte losses or glucose as indicated.
Colloid use is recommended when patients cannot tolerate large crystalloid volumes and overload is of concern. Endogenous albumin is primarily responsible for intravascular osmotic pressure in healthy subjects. However it would appear that controversy still remains about which fluids should be used the crystalloid versus colloid debate.
The paradigm of crystalloid fluids at 10 mLkghr. Crystalloid solutions are mainly used to increase the intravascular volume when it is reduced. This is the first in a series of articles on fluids and electrolytes.
Read the article IV fluids. Doctors may also give people hypertonic fluids before undergoing anesthesia and isotonic. Intravenous therapy abbreviated as IV therapy is a medical technique that delivers fluids medications and nutrition directly into a persons veinThe intravenous route of administration is commonly used for rehydration or to provide nutrition for those who cannot or will notdue to reduced mental states or otherwiseconsume food or water by mouth.
Crystalloid solutions are able to diffuse through capillary wall so there is less fluid that remains in the intravascular space compared to colloid solutions. Thus nonoxygen-carrying fluids eg crystalloid or colloid solutions may be used to restore intravascular volume in mild to moderate blood loss. Crystalloid fluids can be hypotonic isotonic or hypertonic.
Colloid IV Fluids and Solutions Cheat Sheet. For example blood is a colloid. Crystalloid solutions are composed of molecules that can diffuse across cell membranes and can be divided into balanced and non-balanced formulas.
For every 1 mL of approximate blood loss 3 mL of crystalloid solution is given. Remember the 31 rule for crystalloid solutions. Normal saline is one commonly given fluid.
Slowly administer 510 mLkg for dogs and 15 mLkg for cats titrating to effect to minimize the risk of vascular overload. Colloid solutions broadly partitioned into synthetic fluids such as hetastarch and natural such as albumin exert a high oncotic pressure and thus expand volume via oncotic drag. Which IV solution to administer is related to the reason for the fluid loss.
The volumes of study fluids open-label saline and buffered crystalloid solution nonstudy fluids and blood products administered are shown in eTables 3 to 5 in Supplement 2 along with the proportion of patients who received each of these on each study day. Colloids another type of fluid are thicker fluids. There are many clinical factors that may affect the decision to use a crystalloid versus colloid fluid.
Crystalloid fluids move quickly from the intravascular space into other fluid compartments primarily the intracellular compartment. Crystalloids are typically used to replace fluids loss with hemorrhage dehydration and fluid loss due to surgery. In deciding which fluid preparation to use during resuscitation there are two main types of intravenous fluids to choose from either a crystalloid or colloid solution.
Crystalloids are most commonly used and can also treat hyponatremia. Managing phase 1 typically includes administering intravenous fluids often crystalloid or colloid fluid. Less than one-third of the crystalloid volume administered intravenously persists in the vasculature 1 hour after administration 4 making these fluids an excellent choice for treating dehydration and electrolyte derangements and correcting free water deficits.
Colloids given by IV include albumin and dextran. These add fluid to the blood system. Was a synthetic gelatin-based colloid.
It is a crystalloid fluid. Although all IV fluids must be administered carefully hypertonic solutions are additionally risky. A variety of fluids have been recommended for use such as plasma human albumin solution HAS dextran and Hartmanns solution.
If response is inadequate consider IV administration of a colloid such as hetastarch. Pryke S 2004 Advantages and disadvantages of colloid and crystalloid fluids. Crystalloid solutions contain ions with or without glucose whereas colloid solutions contain proteins or high molecular weight polymers that maintain the oncotic pressure of blood once in circulation.
The European Journal of Anaesthesiology publishes original work of high scientific quality including laboratory work of clinical relevance. However an optimal regimen for the use of colloids electrolytes and water after severe burns has not been established. D5W dextrose 5 in water is a crystalloid isotonic IV fluid with a serum osmolality of 252 mOsmL.
Remember youre trying to replenish intravascu-lar volume not deplete the third space. These are fluids that contain minerals such as sodium and are water-soluble or dissolve in water. Crystalloid solutions contain small molecules that flow easily across semipermeable membranes.
However the body increases cardiac output to maintain oxygen delivery DO2 and increases oxygen extraction. Owing to the increased risk of kidney injury colloids should be cautiously used in patients with renal impairment. Crystalloid solutions contain small particles that that pass easily from the bloodstream to cells and tissues.
2
Crystalloids Vs Colloids By James Morgan
Intravenous Fluids Oral Rehydration Solution Dr Ruwan Parakramawansha

Pdf Crystalloids Colloids Blood Blood Products And Blood Substitutes Daniel Low Academia Edu
Fluid Selection Ph Guided Fluid Resuscitation Emcrit Project
Crystalloids Amp Colloids
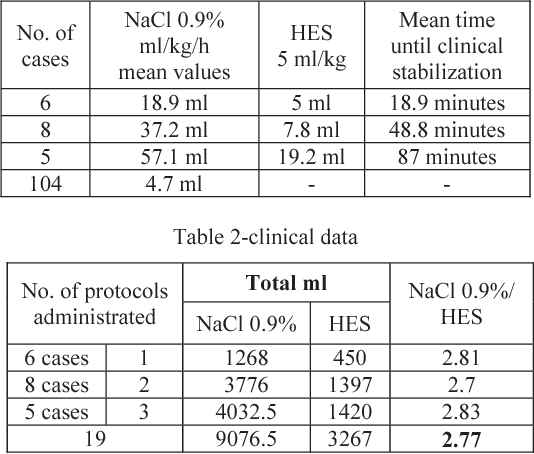
Pdf Crystalloids Colloids Ratio For Fluid Resuscitation During Anesthesia Semantic Scholar

Crystalloids And Colloids Anesthesia Key





